
A Case of Persistent Low Back Pain: Looking Beyond the Painful Area
This case describes a 46-year-old patient who had been struggling with low back pain for nearly five months.
The patient is an active military professional. In early 2025, he became a father for the second time. During the first weeks after the birth, he was frequently getting up at night to help with feeding, soothing and lifting the baby.
One night, while placing his newborn back into the cradle, he felt a sudden sharp pain in his lower back. His back “locked,” and he was unable to move normally for almost a week.
His general practitioner prescribed pain medication and muscle relaxants and referred him to physiotherapy. Within a month he was able to return to work, but the symptoms never fully resolved.
He continued to experience:
stiffness in the lower back
pain around the L3–L4 level
discomfort when lifting or sitting for longer periods
He described the feeling as:
“With every movement, it feels like I’m close to another spasm — like my spine could snap.”
Because of this, he gradually developed a fear of movement.
First Consultation and Clinical Reasoning
This patient came to my clinic in July 2025. At rest, he rated his discomfort as 2/10, increasing to 5–6/10 when:
lifting his baby
carrying weight
sitting for long periods
The pain was localised to the central lower back. However, there was no clear injury or trauma that could explain why the symptoms had lasted for months. When this happens, it is important to look beyond the painful area and explore the patient’s history. One important detail emerged. At the age of 27, the patient had suffered a severe ankle sprain while playing football. The injury involved a ligament rupture and required immobilisation in a cast and later a stabilising boot. Even 20 years later, he still noticed:
weakness in the right ankle
occasional instability
discomfort after running
This information changed the clinical perspective.
Assessment and Hypothesis
There was no primary injury to the spine. But there was a long-standing instability in the ankle. From a fascial and biomechanical point of view, this raised an important question:
Could the body have been compensating for the ankle for years — and could the lower back pain be the final result of that long-term adaptation?
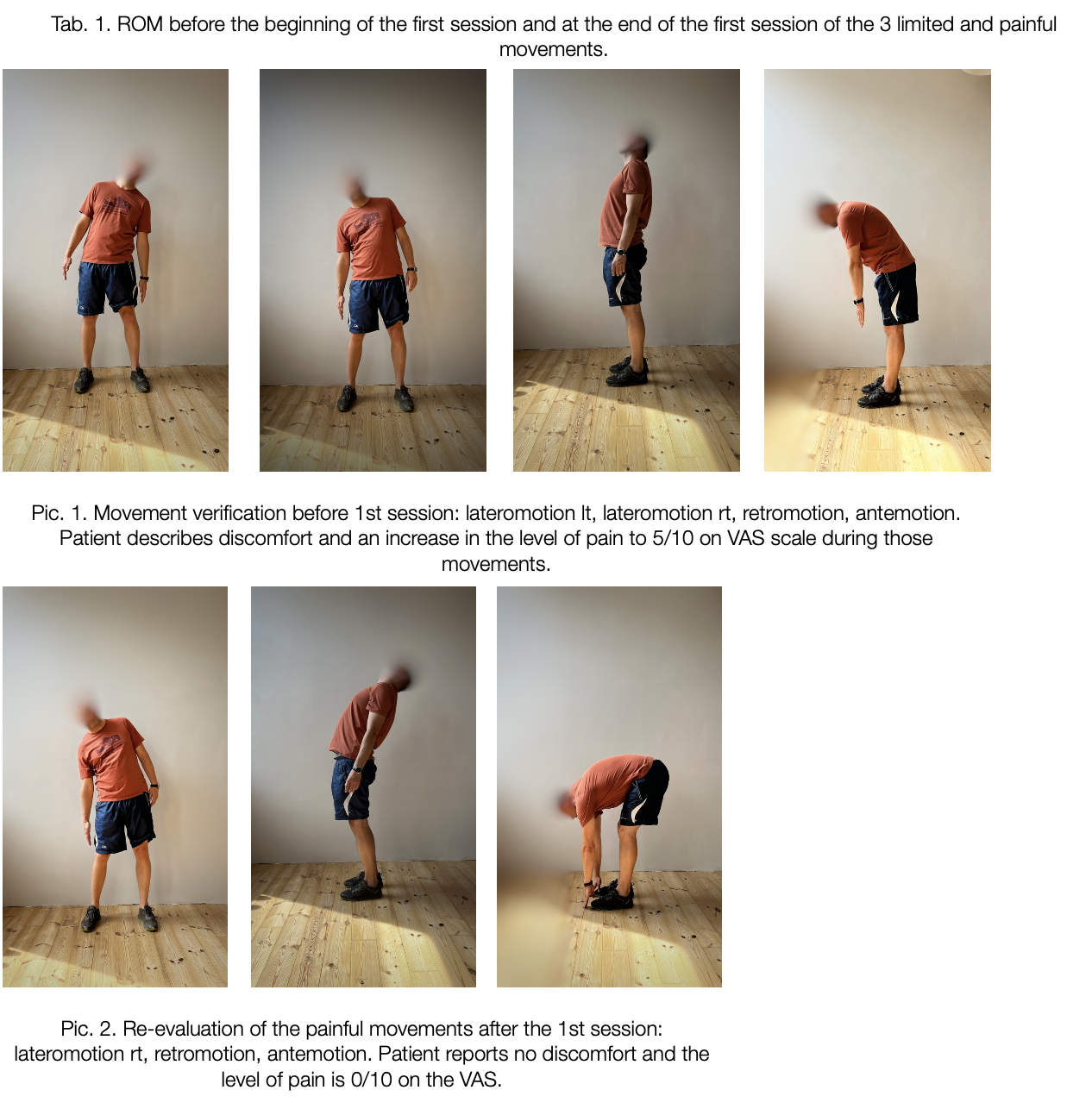
During the assessment:
Single-leg heel raises showed reduced strength and stability on the right side
Forward bending, extension and right side-bending of the spine were limited and felt unstable
Palpation revealed increased tension both in the lumbar area and around the right ankle
This supported the hypothesis that the lower back was not the primary source, but rather a region overloaded by long-term compensation.
Treatment and Progress
Treatment began by addressing fascial densification around the old ankle injury. After working on the first key point:
Forward bending and extension of the spine became pain-free
Side-bending improved
The patient reported more confidence in movement
The heel-raise test immediately felt stronger and more stable
After the second session:
All spinal movements were normal
Fear of movement disappeared
The patient returned to running and gym training without pain
Treatment also addressed connected areas along the fascial system, including:
ankle and heel
pelvic region
shoulder and cervical area
The goal was to restore balanced tension across the system, not only locally.
Why This Case Matters
At first glance, the back pain appeared to start after a simple movement — placing a baby in a cradle. But such a movement alone is unlikely to create long-lasting symptoms. The more likely explanation is:
long-term ankle instability
years of compensation through the fascial system
increased load and fatigue after the birth of the child
a final “breakdown” of compensation in the lower back
In other words:
The painful area was the end point — not the origin.
This case illustrates an important principle in chronic pain: When symptoms persist despite local treatment, the real cause may be located elsewhere in the system.
Understanding the Treatment Approach (Theoretical Framework)
Fascia is a thin but strong layer of connective tissue that surrounds and connects muscles, joints, nerves, and organs throughout the entire body. Rather than working in isolated parts, the body functions as one connected system through this continuous fascial network. For movement to feel smooth and effortless, the different layers of fascia need to glide easily over one another. The fascia contains a gel-like substance that helps these layers slide. However, after an injury, surgery, prolonged immobilisation, or repeated strain, this substance can become thicker and less fluid. When this happens, the fascia may become stiff — a change sometimes referred to as densification. When fascia loses its ability to glide normally:
Movement may feel restricted or “tight”
Certain areas may take on extra strain
Other parts of the body may compensate to keep you moving
Over time, these compensations can place increased stress on areas far away from the original problem.
Fascial Manipulation® is a manual therapy approach that aims to restore normal movement within this fascial network. During treatment, the therapist identifies specific points where the fascia feels stiff or restricted. Deep, targeted friction is then applied to these areas to help improve the fluidity of the tissue and restore its ability to slide.
An important principle of this method is sometimes described as “old is gold” — meaning that past injuries, even from many years ago, can still influence how the body moves today. In some cases, the source of the problem may not be where the pain is felt.
Discussion
This case highlights how long-standing movement changes in one part of the body may contribute to pain elsewhere. The patient’s lower back pain did not begin after a clear injury to the spine. Instead, the assessment revealed long-term instability in the right ankle following a severe sprain nearly 20 years earlier. When a joint does not function optimally, the body often adapts by shifting load and movement patterns. These adaptations can travel through the body over time, increasing strain in other areas. Research shows that the deep fascia forms continuous connections from the legs to the lower back. This means that stiffness or altered movement in the ankle may influence how forces are transferred up the body during daily activities such as standing, walking, or lifting.
In this case, several factors likely contributed to the onset of symptoms:
Long-standing ankle instability
Increased physical demands from caring for a newborn
Fatigue and reduced sleep
Gradual build-up of tension along the movement chain
Rather than a single movement causing injury, the episode of back pain may have represented a point where the body’s ability to compensate was exceeded. Another important aspect was the patient’s fear of movement. Chronic pain often leads people to worry that normal movements might cause further damage. When the patient experienced immediate improvement after treatment — and could move without pain — this reassurance helped reduce fear and increased confidence in movement. Addressing both physical and psychological factors is important in long-term recovery from low back pain.
It is also important to interpret these results carefully. This is a single case report, and improvements may be influenced by multiple factors, including the natural course of recovery and the effects of hands-on care and patient expectations. In addition, while Fascial Manipulation® shows promising clinical results, high-quality research studies are still limited.
For clinical practice, this case reinforces several key points:
Chronic low back pain does not always originate in the lower back itself
A detailed history of previous injuries can provide valuable clues
Assessing the whole movement system, including distant joints, may improve treatment planning
Hands-on treatment may be most effective when combined with exercise and education
Following the restoration of pain-free movement, the patient began a gradual return to strengthening and functional exercise to support long-term stability and reduce the risk of recurrence.
Continue learning
If you’d like to better understand the difference between acute and chronic conditions and why local treatment doesn’t always bring lasting results:
→ Read the article:
Why Local Treatment Doesn’t Always Work in Chronic Cases
If you prefer a video explanation of the same concepts:
→ Watch on YouTube:
When Pain Location Is Not the Source – Understanding Chronic Pain
References:
Celik, D., Yeldan, İ., & Yazıcı, A. G. (2019). The relationship between myofascial trigger points and clinical outcomes in patients with chronic low back pain. Journal of Bodywork and Movement Therapies, 23(1), 63–67. https://doi.org/10.1016/j.jbmt.2018.12.001
Costa, L. D. C. M., Maher, C. G., McAuley, J. H., Hancock, M. J., Herbert, R. D., & Costa, L. O. P. (2012). Prognosis for patients with chronic low back pain: Inception cohort study. BMJ, 345, e4393.https://doi.org/10.1136/bmj.e4393
Cowman, M. K. (2015). Hyaluronan and hyaluronan fragments. Advances in Carbohydrate Chemistry and Biochemistry, 72, 1–59. https://doi.org/10.1016/bs.accb.2015.08.001
Goubert, L., Crombez, G., & De Bourdeaudhuij, I. (2017). Low back pain, disability and physical activity: The role of pain-related fear. Pain, 157(1), 173–179. https://doi.org/10.1097/j.pain.0000000000000368
Hagiwara, Y., Ando, A., Ohta, R., Itoigawa, Y., & Sekiguchi, T. (2024). Association between ankle functional instability and nonspecific low back pain: A cross-sectional study. Journal of Orthopaedic Science, 29(2), 303–309. https://doi.org/10.1016/j.jos.2023.06.001